-
Annovis Bio Announces Statistically Significant Phase II/III Data in Patients With Early Alzheimer’s Disease
المصدر: Nasdaq GlobeNewswire / 29 أبريل 2024 10:10:00 America/New_York
- Significantly higher rate of improvement in ADAS-Cog 11 scores in each treatment dose relative to placebo for patients with mild AD
- Improvement in cognition measured by ADAS-Cog 11 at three months is 3.3 points as compared to 0.3 for placebo, consistent with our previous Phase II AD/PD and Discover studies
- Plasma Tau protein levels are reduced, consistent with our previous Phase II biomarker data
- Based on the findings of this symptomatic study, Annovis plans to conduct a pivotal disease-modifying Phase III trial in biomarker-positive early AD patients
MALVERN, Pa., April 29, 2024 (GLOBE NEWSWIRE) -- Annovis Bio, Inc. (NYSE: ANVS) (“Annovis” or the “Company”), a clinical-stage drug platform company developing novel therapies for neurodegenerative diseases, such as Alzheimer’s (AD) and Parkinson’s disease (PD), today announced the data from its Phase II/III Alzheimer study of buntanetap in mild to moderate AD patients. Based on these data, the Company plans to conduct a pivotal Phase III trial in biomarker-positive early AD patients.
Buntanetap is an oral molecule that selectively binds to an iron-responsive element in the mRNA of amyloid precursor protein (APP) and other neurotoxic proteins and inhibits their translation. Through this mechanism, buntanetap was shown to decrease the production of amyloid beta (Aβ), tau, alpha-Synuclein (αSYN), and TDP43.
Phase II/III Study
The Phase II/III study was a randomized, double-blind, placebo-controlled trial investigating the efficacy, safety, and tolerability of buntanetap in patients with mild to moderate AD. This was a dose-ranging study where patients received either one of three doses of buntanetap (7.5mg, 15mg, or 30mg) or placebo on top of their standard of care for 12 weeks. In this study, over 700 patients were screened, a total of 353 patients were enrolled, and 325 patients completed the study across 54 sites in the US. The study included mild to moderate AD patients whose Mini Mental State Examination (MMSE) scores at baseline ranged from 14 to 24. More information on the trial can be found on www.clinicaltrials.gov (NCT05686044).Beyond safety, the trial assessed the changes in two co-primary endpoints: Alzheimer’s Disease Assessment Scale-Cognitive Subscale 11 (ADAS-Cog 11) and Alzheimer’s Disease Cooperative Study Clinician’s Global Impression of Change (ADCS-CGIC), which assess cognition and activities of daily living. The study monitored for safety and collected plasma to measure several biomarkers to assess the disease state, potential disease progression, and treatment effects.
ADAS-Cog 11 (Co-primary Endpoint) Shows a 3.3 Statistically Significant Improvement
We observed a significantly higher improvement in ADAS-Cog 11 scores in each treatment dose relative to placebo for patients with mild AD. The analysis focused on biomarker-positive early AD patients (MMSE 21-24, pTau217/tTau≥4.2%) found that ADAS-Cog 11 was highly statistically significant at all 3 dose levels and in the combined dose levels compared to placebo as well as to baseline (Figure 1). This objective measure of cognitive function confirms our findings from the two small Phase II studies that showed improvement in cognition in mild AD patients (Fang et al. JPAD 2023). The treatment response in the current study was not related to a patient’s age or sex.Note 1: AD biomarker field has fast accelerated in the past few years. When we initiated the study in January 2023, the gold standard for measuring Alzheimer’s-related amyloid and tau biomarkers were CSF and PET scans. Clinically validated plasma biomarkers became commercially available in 2024 and have been shown to be similar or superior to CSF biomarkers (Ashton et al. JAMA 2024, Barthelemy et al. Nat. Med 2024, Meyer Alzheimer’s Dement 2024).
Note 2: Our initial recruitment did not prescreen patients for AD biomarkers in plasma. When we became aware of issues from other AD studies with sites recruiting non-AD patients, we fast-tracked biomarker measurements by collaborating with C2N Diagnostics. This enabled us, when we unblinded the data, to tell which patients had confirmed AD and which did not (Ashton et al. JAMA 2024, Barthelemy et al. Nat. Med 2024, Meyer Alzheimer’s Dement 2024). Out of 325 patients who completed the Phase II/III trial, 202 had a ratio of pTau217/tTau≥4.2% that indicates AD. We further subdivided the patient population into moderate (MMSE 14-20; 112 patients) and mild (MMSE 21-24; 90 patients) AD patients. These two selections were not pre-specified analyses.
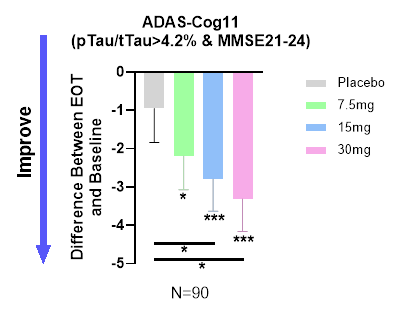
Figure 1. Dose-dependent improvement in cognition in the population with confirmed early AD.
At the end of 3 months of treatment, placebo group demonstrated slight improvement (LSM(SE), 0.26 (0.91)), but not significantly different from baseline. All three buntanetap treatment groups showed statistically significant improvement from their corresponding baseline (7.5mg improved 2.19 (0.87), p=0.013; 15mg improved 2.79 (0.81), p=0.001; 30mg improved 3.32 (0.82), P<0.001). Both 15mg and 30mg treatment groups also had a statistically significant improvement relative to placebo group (p=0.042 and 0.015 respectively). EOT- End of Treatment * P<0.05; ** P<0.01; ***P<0.001
Treatment Response is Highly Correlated to MMSE Score at Baseline
When we subdivided the baseline MMSE scores for patients positive for AD according to their pTau217/tTau >4.2% ratio, we observed a dose-dependent relationship to MMSE at baseline – the response to buntanetap treatment is more pronounced in mild AD patients than in those with more advanced AD. The response in the 30mg dose treatment group R2=0.17 (R² or the coefficient of determination), p<.001, indicates statistical significance of the MMSE score, which was not evident in the placebo group. Figure 2 confirms the efficacy of buntanetap as previously shown in Figure 1.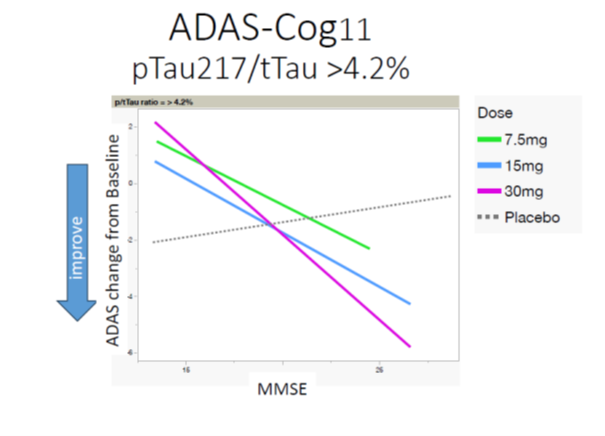
Figure 2. Buntanetap’s efficacy is strongly correlated with MMSE status.
Three-Fold Increase in Number of Responders in Treatment Group vs. Placebo
A further look at responders versus non-responders showed a dose-dependent increase in the number of responders from placebo to 30mg. There was a three-fold difference in the proportion of participants who improved in the 30mg group relative to placebo (Table 1).Responders vs Non-Responders Dose Responders
(Number & Percentage)Non-Responders
(Number & Percentage)Total Number Placebo 6 (27.27%) 16 (72.73%) 22 7.5mg Buntanetap 14 (73.68%)** 5 (26.32%) 19 15mg Buntanetap 18 (72.00%) ** 7 (28.00%) 25 30mg Buntanetap 21 (87.50%)*** 3 (12.50%) 24 **Contrast with Placebo, p value < 0.01, *** Contrast with Placebo, p value < 0.001
Table 1. Distribution of responders and non-responders in placebo and 3 doses of buntanetap.
Data presented in Figures 1, 2 and Table 1 demonstrate the efficacy of buntanetap in early AD patients.
Other Study Endpoints
ADCS-CGIC
This study was designed to enroll 80 patients per group with minor expectations for a statistically significant outcome in ADCS-CGIC or ADCS-ADL. We measured both endpoints to assess a possible trend that could support a power analysis for the sample size in the next disease-modifying 18-month study.During the trial, ADCS-CGIC in all groups of patients barely changed, with no statistically significant difference observed. The 15mg and 30mg buntanetap groups slightly improved in mild AD patients. The subjective nature of this assessment allowed for a greater placebo effect, particularly in the advanced Alzheimer's population, as patients and caregivers were likely hopeful for change.
ADCS-ADL
We observed a large placebo effect in ADCS-ADL, with 15mg and 30mg buntanetap groups showing similar improvements with no statistical difference between the groups.Biomarkers
In accordance with the mechanism of action of buntanetap, we observed a reduction in plasma tTau (total Tau) after treatment, providing further credence to buntanetap’s efficacy and mechanism of action (Figure 3).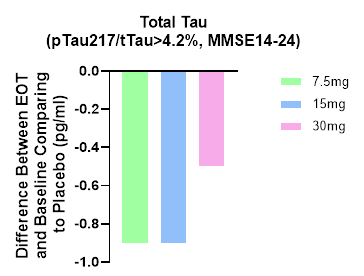
Figure 3. Total Tau levels are decreased at all 3 doses, which is consistent with our earlier Phase IIa data, where we also saw a decrease in tTau (Fang et al. JPAD 2023).
We plan to measure additional biomarkers for inflammation and axonal and synaptic functions.
Safety and Tolerability
Buntanetap was very well tolerated. The safety profile observed in this study was consistent with prior clinical trials, with comparable numbers of adverse events (AEs) between treatment and placebo groups. The majority of reported AEs were mild to moderate in severity. No serious AEs were related to buntanetap.Summary
- Buntanetap, a once-daily oral medicine with an exquisite safety profile, improves ADAS-Cog 11 score in a dose-dependent fashion to the mean of 3.3 points. The data is highly statistically significant in a subpopulation of early AD patients, confirmed by multiple data and biomarker analyses
- Efficacy strongly correlates with disease stage at entry (as measured by MMSE)
- Efficacy in the CGIC endpoint was not reached due to the limited number of patients and short trial duration
- In accordance with the mechanism of action, buntanetap lowered tTau levels, suggesting a disease-modifying effect
- As seen in all previous studies, buntanetap is safe and well tolerated.
Next Steps
This short study shows a symptomatic effect with a possible disease-modification trend according to the tau data. The next study will have a longer duration, improved design and be statistically powered to validate symptomatic improvement and disease-modification.Annovis will report the data to the FDA and ask for an end-of-Phase II meeting. We expect to discuss the data with the FDA in the next two to three months and then move on to the next Phase III study to confirm and expand these findings in an 18-month disease-modifying trial focusing on biomarker-positive early AD patients. We further plan to present the data at the AAIC2024 and to publish it in a peer-reviewed journal.
Kore Liow, MD, Director, Memory Disorders Center, Alzheimer's Research Unit, Clinical Professor of Neurology, University Hawaii, a Principal Investigator who conducted all four Phase II and III studies in Alzheimer’s and Parkinson’s disease, commented:
“These findings are a significant milestone for Alzheimer's patients. Buntanetap has the potential to be the first safe and convenient oral therapy that provides symptomatic efficacy while slowing disease progression. The mechanistic pathway and science are novel, and our physicians and researchers at the Hawaii Memory Center & Alzheimer's Research Unit are proud to have contributed to four studies and look forward to participating in future studies.”Melissa Gaines, SVP, Clinical Operations, and Cheng Fang, PhD, SVP, Research & Development, at Annovis Bio added:
“This Phase II/III Alzheimer study builds and expands on the understanding we collected in the Phase II studies. Based on buntanetap’s unique mechanism of action, we believe it can give patients both symptomatic and disease-modifying benefits. It’s really exciting to see that this study confirmed what we have observed in the previous Phase II studies in both the improvement of patients’ cognition and the improvement of biomarkers. We are unaware of any double-blind, placebo-controlled studies demonstrating this level of improvement in the ADAS-Cog 11 after one and after three months. We are preparing the data to discuss with the FDA on how to proceed to show disease-modification, for presentation at AAIC2024 and for publication.”About Buntanetap
Buntanetap (formerly known as Posiphen or ANVS401) attacks neurodegeneration by inhibiting the formation of multiple neurotoxic proteins - amyloid beta, tau, alpha synuclein, and TDP43 - thereby improving synaptic transmission, axonal transport and neuroinflammation. Dysregulation of these pathways has been shown to be the cause of nerve cell degeneration and ultimately death. By attacking these pathways, buntanetap has the ability to reverse neurodegeneration in AD, PD, and other neurodegenerative diseases.About Annovis Bio, Inc.
Headquartered in Malvern, Pennsylvania, Annovis Bio, Inc. is a clinical-stage, drug platform company addressing neurodegeneration, such as Alzheimer’s Disease (AD), Parkinson’s Disease (PD), and other chronic neurodegenerative diseases. The company believes it is the only company developing a drug for both AD and PD designed to inhibit more than one neurotoxic protein to restore axonal and synaptic activity. By improving brain function, the Company’s goal is to treat memory loss and dementia associated with AD as well as body and brain dysfunction associated with PD. For more information about Annovis Bio, please visit the Company's website www.annovisbio.com and follow us on LinkedIn and Twitter.Forward-Looking Statements
This press release contains "forward-looking" statements within the meaning of Section 27A of the Securities Act of 1933, as amended, and Section 21E of the Securities Exchange Act of 1934, as amended. All statements other than statements of historical fact are statements that could be deemed forward-looking statements. The Company advises caution in reliance on forward-looking statements. Forward-looking statements include, without limitation, the Company's plans related to clinical trials. These statements involve known and unknown risks, uncertainties and other factors that may cause actual results to differ materially from those implied by forward-looking statements, including regarding patient enrollment, the effectiveness of buntanetap and the timing, effectiveness, and anticipated results of the Company's clinical trials evaluating the efficacy, safety, and tolerability of buntanetap. See also additional risk factors set forth in the Company's periodic filings with the SEC, including, but not limited to, those risks and uncertainties listed in the section entitled "Risk Factors," in the Company's Annual Report on Form 10-K and Quarterly Reports on Form 10-Q filed with the SEC. All forward-looking statements in this press release are based on information available to the Company as of the date of this filing. The Company expressly disclaims any obligation to update or alter its forward-looking statements, whether as a result of new information, future events or otherwise, except as required by applicable law.Investor Contacts:
Maria Maccecchini, Ph.D.
maccecchini@annovisbio.comReferences:
1. Fang C, Hernandez P, Liow K, Damiano E, Zetterberg H, Blennow K, Feng D, Chen M, Maccecchini M. Buntanetap, a Novel Translational Inhibitor of Multiple Neurotoxic Proteins, Proves to Be Safe and Promising in Both Alzheimer's and Parkinson's Patients. J Prev Alzheimer’s Dis. 2023;10(1):25-33. doi: 10.14283/jpad.2022.84. PMID: 36641607.
2. Ashton NJ, Brum WS, Di Molfetta G, et al. Diagnostic Accuracy of a Plasma Phosphorylated Tau 217 Immunoassay for Alzheimer Disease Pathology. JAMA Neurol. 2024;81(3):255–263. doi:10.1001/jamaneurol.2023.5319
3. Barthélemy, N.R., Salvadó, G., Schindler, S.E. et al. Highly accurate blood test for Alzheimer’s disease is similar or superior to clinical cerebrospinal fluid tests. Nat Med 30, 1085–1095 (2024). https://doi.org/10.1038/s41591-024-02869-z
4. Meyer MR, Kirmess KM, Eastwood S, et al. Clinical validation of the PrecivityAD2 blood test: A mass spectrometry-based test with algorithm combining %p-tau217 and Aβ42/40 ratio to identify presence of brain amyloid. Alzheimer's Dement. 2024; 1-14. https://doi.org/10.1002/alz.13764
Figures accompanying this announcement are available at:
https://www.globenewswire.com/NewsRoom/AttachmentNg/28dd23e3-bb6c-49e2-9522-4d4c894d934c
https://www.globenewswire.com/NewsRoom/AttachmentNg/5a4e081c-a8e3-46c1-8b76-e890aa18cd40
https://www.globenewswire.com/NewsRoom/AttachmentNg/da92d14a-c0b5-4ce9-8cdc-99830d75c078

Figure 1
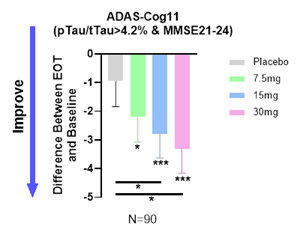
Dose-dependent improvement in cognition in the population with confirmed early AD.
Figure 2
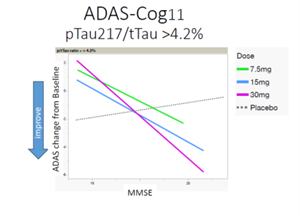
Buntanetap’s efficacy is strongly correlated with MMSE status.
Figure 3
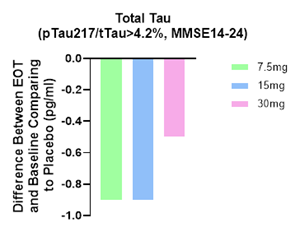
Total Tau levels are decreased at all 3 doses, which is consistent with our earlier Phase IIa data, where we also saw a decrease in tTau (Fang et al. JPAD 2023).